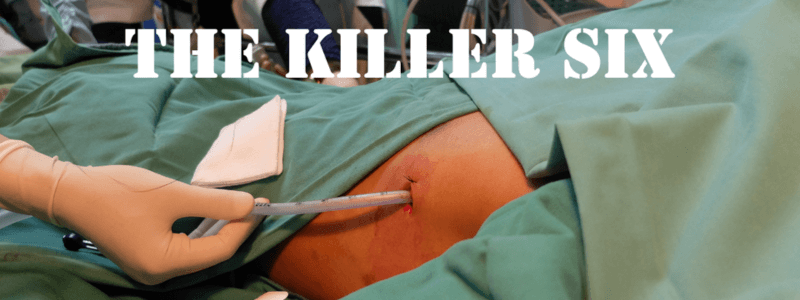
Arterial line placement is a very common procedure in critical care and emergency medicine settings. The most common indications are:
- Haemodynamic instability requiring continuous direct BP monitoring
- Titration of vasopressors (or other cardioactive drugs)
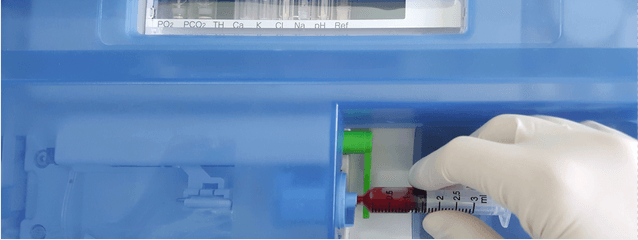
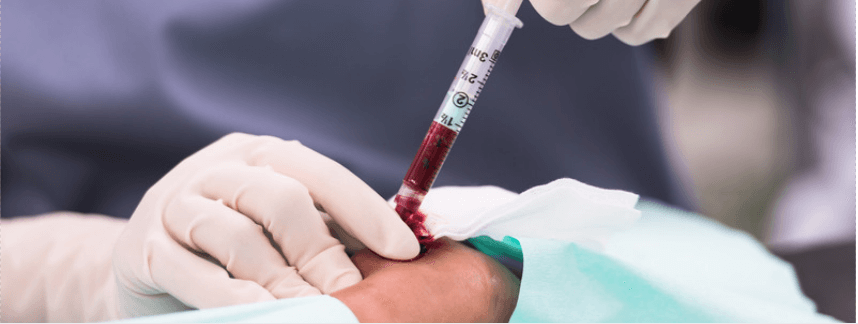
- Need for recurrent or serial arterial blood gas analysis
Radial arterial lines
The most common site used for arterial cannulation is the radial artery. The radial artery has several advantages, including:
- Superficial nature of the radial artery makes it easily located
- Peripheral location of the site means it can be easily maintained
- The anatomy is consistent between individuals
- There is a low complication rate at this site
The radial artery can be located by palpating the radial artery at the wrist just proximal to the flexor crease. The puncture site should be at least 1 cm proximal to the styloid process to prevent puncture of the flexor retinaculum and the small superficial branch of the radial artery. It is advisable to perform the initial puncture as distal as possible in case multiple attempts at arterial cannulation are required.
Allen’s test
The modified Allen’s test (often referred to as simply Allen’s test) is a commonly cited, and frequently performed test that looks for abnormal circulation in the hand. It is most commonly performed prior to sampling or cannulation of the radial artery at the wrist.
The hand receives a joint blood supply from the ulnar and radial arteries.Within the hand two arterial networks form between these two arteries and their branches:
- The deep palmar arch:this is formed predominantly by the terminal part of the radial artery, with the ulnar artery contributing via its deep palmar branch by an anastomosis. It lies on the bases of the metacarpal bones and the interossei and is covered by adductor pollicis, the flexor tendons and the lumbricals. The palmar metacarpal arteries arise from the deep palmar arch.
- The superficial palmar arch:this is formed predominantly by the ulnar artery, with a contribution from the superficial palmar branch of the radial artery. It is found anteriorly to the flexor tendons in the hand, but just deep to the palmar aponeurosis. The common palmar digital arteries and four digital branches arise from the superficial palmar arch.
The deep and superficial palmar arches connect via an anastomosis. The patency of this anastomosis can be tested via Allen’s test.
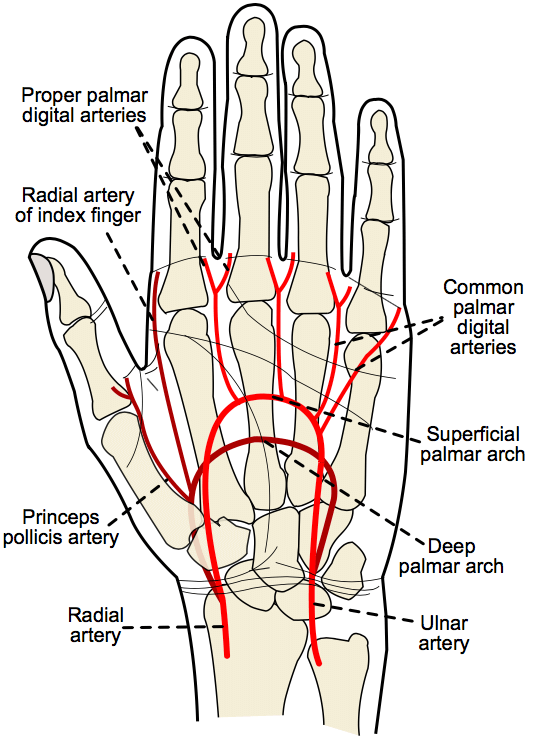
The arterial supply of the hand
The modified Allen’s test is performed as follows:
- The hand is elevated, and the patient asked to clench their fist for 30 seconds
- Pressure is then applied over both the radial and ulnar arteries simultaneously, occluding both vessels
- The hand is then opened while still elevated, and should now appear pale and blanched
- The pressure over the ulnar artery is now released, but the pressure maintained over the radial artery
The colour should return within 5-15 seconds, and if it fails to do so, this suggests that the arterial supply to the hand from the ulnar artery is insufficient for the ABG to be performed.
Femoral arterial lines
The femoral artery is the second most common site for arterial cannulation. It is less convenient than the radial artery for maintenance and has a higher risk of infection, but is larger than the radial artery, has a stronger pulse, and has lower risks of thrombosis. Overall both the radial and femoral sites perform well, and when considering the optimal site for placement the risks and benefits should be considered on a patient-by-patient basis.
The femoral artery can be located just distal to the midpoint of the inguinal ligament, midway between the anterior superior iliac spine and the pubic tubercle. Here it lies medial to the femoral nerve and lateral to the femoral vein and lymphatics.
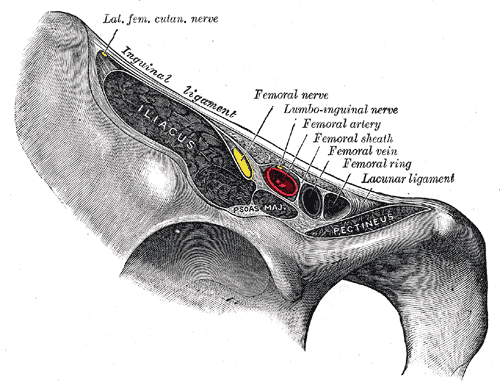
The anatomical location of the femoral artery at the mid-point of the inguinal ligament (from Gray’s Anatomy)
Methods for insertion
The two main methods for the placement of arterial lines are:
- The “over-the-needle” technique
- The “over the wire” technique (Seldinger technique)
The “over-the-needle” technique is performed as follows:
- Gently palpate the pulse with the non-dominant hand to guide the placement of the needle
- Insert the needle at a 30-45 degree angle to the skin
- Advance the needle until a pulsatile blood flash is seen in the chamber/catheter
- Reduce the angle of the catheter to 10-15 degrees to the skin
- Then advance the catheter over the needle into artery
The “over-the-wire” technique is performed as follows:
- Gently palpate the pulse with the non-dominant hand to guide the placement of the needle
- I Insert the needle at a 30-45 degree angle to the skin
- Advance the needle until a pulsatile blood flash is seen in the chamber/catheter
- Insert the wire through the needle into the artery
- Remove the needle and advance the catheter over the wire into the artery

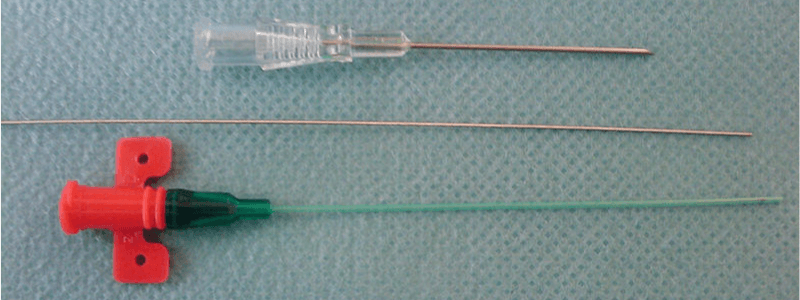
A typical Seldinger set, image sourced from Wikipedia
Courtesy of Arif Najafov CC BY-SA 3.0
Ultrasound guidance is an extremely helpful adjunct and should be considered in all arterial line placements. The use of ultrasound has been shown to significantly increase the success at first attempt at placement and also to decrease the time taken to successfully site the catheter.
Once the arterial line has been sited the arterial line transducer set must be set up.
Contraindications and complications
As with any procedure, it is essential to have a good understanding of the contraindications and possible complications.
Absolute contraindications for arterial line placement include:
- Absent pulse
- Thromboangiitis obliterans (Buerger disease)
- Raynaud’s syndrome
- Full-thickness burns at placement site
- Known arterial insufficiency or occlusion distal to placement site
- Traumatic or vascular injury proximal to placement site
Relative contraindications for arterial line placement include:
- Anticoagulation or coagulopathy
- Atherosclerosis
- Inadequate collateral flow
- Infection overlying placement site
- Partial-thickness burns at placement site
The main complications associated with the placement of arterial lines are as follows:
- Bleeding
- Puncture site haematoma
- Local infection
- Line sepsis
- Temporary arterial occlusion
- Permanent arterial occlusion (rare)
- Pseudoaneurysm formation