The Emergency Medicine training post interview is a source of great anxiety for many candidates. This interview is the final stage before gaining a UK training post that will run through to Consultant level.
In this month’s post, Dr. Usama Basit shares his experience, and some invaluable advice, based on his interview last year.
My interview was last year and was for an ACCS-EM run through training post. It was my first major interview experience in the UK. As the interview was last year, some of the details are a bit sketchy, but this is how I remember the events of the day.
There were two batches of interviews held on the day, one in the morning, and one on the afternoon, and I took part in the morning batch. I believe that there were also other days on which interviews were held.
The interview was comprised of four stations:
- Station 1: Presentation
- Station 2: Ethical/clinical scenario
- Station 3: Portfolio assessment
- Station 4: General Management etc
There were two Emergency Medicine consultants present at each station, so in total, eight consultants assess you and allocate a score.
Station 1
My first station, and possibly worst one, was the presentation station. In this station, you are allocated a topic for presentation. The topic can be about pretty much anything, as long as it is remotely related to the medical field, and it doesn’t have to be clinical.
After reaching the station, you are allocated a topic and given a few minutes to prepare (3 or 5 minutes, I don’t remember the exact amount of time). You are then taken into a separate room, provided with different coloured marker pens, and some sheets of paper on a stand. My topic was ‘Should the UK adopt a policy of implied consent for organ donation after death?’ This required some serious thought on my part, and it took a few moments to fully understand the meaning of the statement. My interpretation of this statement was that it is asking if the UK should adopt a policy of implied consent where the wishes of the deceased are not known, in cases of sudden or unexpected death, and utilise their organs without actually having their prior consent.
I decided that I stood against this notion, and started to prepare a presentation based on this stance. Now here is where I hit a snag, it is easy to decide if you support or oppose a policy, but making a 5-7 minute presentation is far more challenging. What should I do? I started by outlining what I wanted to speak about; the first minute was an introduction explaining organ donation is, which organs can be transplanted and used by other individuals, etc. I then tackled the controversial topic: yes or no. I said no, and then stated my reasons: patients should ultimately have the right to decide what happens to them and their bodies, and in cases where they cannot, or have not expressed their wishes, then their next of kin, legal guardian, or court-appointed person has to make the decision for them. But someone has to MAKE the decision for this to happen; it shouldn’t automatically happen, you have to take into account the deceased person’s wishes, their family’s wishes, and the religious or cultural factors influencing their decision. I babbled on for a while, and then eventually petered to a stop. The two consultants present in the room smiled at me.
I thought that was it. But, no, they had questions! The first examiner was pleasant and smiling. She asked me a question that I, unfortunately, cannot remember. I did not know the answer to that question, but I bravely said I could look up the information if you like and come back to you with an answer, but that I honestly did not know. This seemed to be enough for her, and she didn’t ask me any further questions.
The second consultant approached me quite differently and applied lots of pressure! I quickly realised that they were playing good cop, bad cop. He questioned my opinion, asked me three times how I felt it was appropriate to let organs go to waste when the dead people couldn’t utilise them and why would I not want these to be put to good use. I kept calm and reiterated my initial stance; he even banged his hand on the table to express his displeasure at my answer. I stood my ground, what else could I do, I did not want to portray one opinion from the beginning of the presentation and then back down and go for the complete opposite opinion. He finally smiled at me and said: “your time is up, you may proceed to the next station.” I was shaking in my suit, but I felt it could have gone worse, I had at least had the opportunity to express my opinions.
Station 2
My second station was the ethical/clinical scenario station. There were two consultants at this station, each presenting one scenario, but both were sat at the same table and assessed both scenarios.
The first case was the ethical case: “You are asked to see a 50-year-old male in Resus who has presented clutching his chest in severe pain. He speaks no English, and you do not speak his language. He is accompanied by his daughter, who is approximately 11 or 12 years old, and who speaks both languages fluently. How will you proceed?”
Having now worked in UK Emergency Departments for a while, I knew that it was frowned upon to use relatives or friends as interpreters. Instead, the use of Hospital provided professional interpreters, or phone-based services, such as ‘language line’ are preferred. While these options aren’t the most practical solution, I think it was the answer they wanted.
I explained that I would ideally like to use a professional interpreter or ‘language line’, but since this is potentially an Emergency, and I am aware of the time it may take to arrange an interpreter, I would at least like to ask for patient’s known history, whether he was allergic to anything, and start the process of giving painkillers and making an assessment with his consent via his daughter. I also used the phrase “I will ask my seniors to advise me on this situation as well,” which always sits well with examiners, especially when interviewing for more junior posts. They do not want you to be a hero; they want you to be safe and utilise appropriate senior help whenever you feel the situation entails.
The consultant then asked me if there was any other avenue I could utilise for this purpose, and I remembered once having had to use one of our staff members, a registered nurse, as an interpreter. I mentioned that which was seemingly the right answer, as they moved on to the next question: “What problems do you think that you may face if you do end up using the daughter as an interpreter? I explained that she is not a professional and that there is no guarantee that she will be able to relay the stream of information to and from the patient accurately. I also mentioned there would be aspects of the history that she may not be aware of, such as his medications, or a health condition, such as a malignancy, that he has kept from her. She may also be terrified and seeing her father in pain or unwell may cause her to become distressed, and using her as a translator could make this worse.
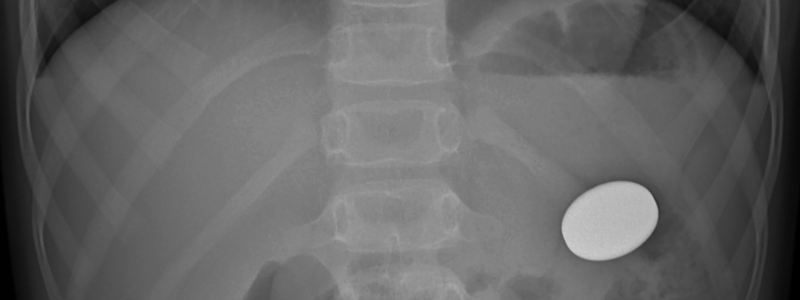
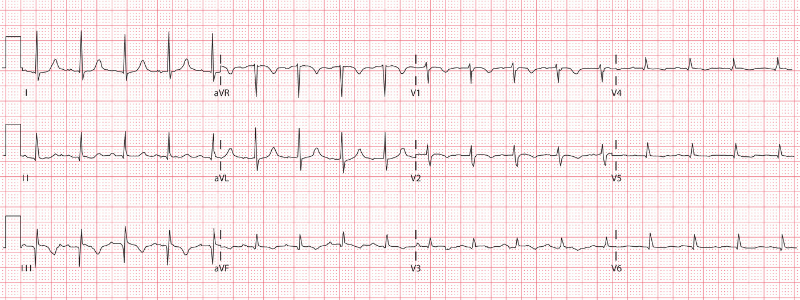
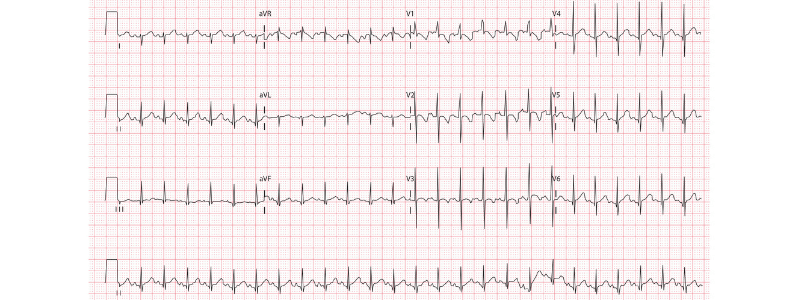
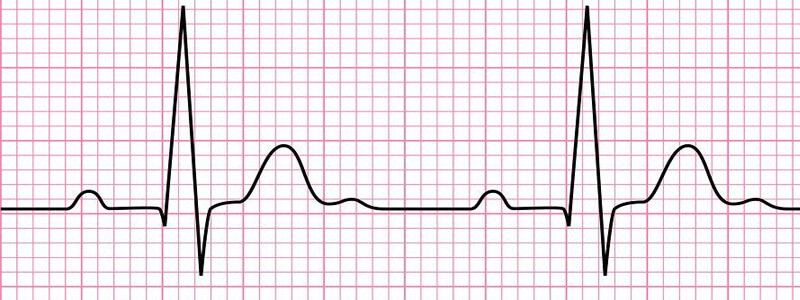
The buzzer went off at this point, and I was asked to move on to the next examiner. The second scenario was a clinical case in which the interviewer showed me an ECG and asked me to identify the abnormality. I felt that the ECG appeared to demonstrate an SVT, and she then she went on to ask me how I would go about managing the patient. I kept giving her options but felt she was probing further, and then it clicked: ask for senior help or specialist advice, which I mentioned, and she then seemed happy with my answer. The second station then ended, and I moved on to station number 3.
Station 3
My third station was the portfolio station. Once again there were two interviewers, who already had access to my portfolio. We were asked to submit our physical portfolios outside the station at the start of the interview, and before our turn came, they had already gone through the broader aspects of each portfolio.
It is worth mentioning at this point that there were candidates who had come to the interview armed with huge binders of information. One candidate had three folders and seven rolls of what seemed like large maps, but were very likely poster presentations of research and audits that he had undertaken. These candidates greatly unnerved me and the other candidates that only brought a single thin portfolio! Anyway, I went in, they asked me a few fairly predictable questions that mostly seemed aimed at confirming information that was already provided in the application and portfolio.
The sorts of questions I was asked include: “So you have done an ALS course, but no others, correct?” – Yes. “And you have no other degrees other than your primary medical qualification?” – Yes. “And I see you have some feedback from medical students that you have taught.” – Yes. “Is there any other evidence of teaching? – No.
Things went on very much in this fashion until we discussed a few aspects of my CV. I was asked about prior experience: “Tell me about this 6-month volunteer post you did back in the USA”, and “So, I see you have some experience in Oncology? Tell me more.”
This station felt like a general chat to gain an idea of who I am, what I have done, and how I have turned into this person sitting in front of them, applying for a training post in Emergency Medicine. It was certainly less stressful than the other three stations.
Station 4
Finally, I moved on to my fourth and final station. This station had something of a management feel to it, and the questions were aimed more at management type scenarios than clinical ones.
They asked me if I knew what the term “exit block” meant. I didn’t, so they explained that an exit block means that patients are coming into the Emergency Department, but are not leaving it, probably due to a shortage of beds for admitted patients. In effect, the system isn’t moving forward, and there is a jam or a literal block. They then asked me how I would deal with this phenomenon. I thought about it and replied that I would “Make sure it’s still a safe department, make sure everyone has adequate pain relief, next antibiotic doses, and regular medications prescribed. If patients had been waiting in the department for a long while, I would attempt to get them into a more comfortable bed instead of the trolley, try to offer them something to eat if it is clinically warranted, and a cup of tea or coffee would go a long way, along with a sincere apology about the wait and an explanation that all efforts are being made to make sure things progress.”
There was another question, which I can’t accurately remember, but I think it was along the lines of “If you see a colleague that is drunk or intoxicated, how would you proceed?” I answered as best as I could.
That was it. I then went home, or rather I went to the train station, and took 3 connecting trains back home, slept for 3 hours and went to work on a night shift.
I left feeling as though I hadn’t done too well, but fortunately, I was successful in my application, and I am now a fully-fledged Emergency Medicine trainee! My next interview will be for a consultant post in at least six years time.
Header image used on licence from Shutterstock
Medical Exam Prep would like to thank Dr. Usama Basit for contributing this post.
Dr. Basit is an Emergency Medicine trainee in the UK. He writes about his own personal experiences as a blog series, which can be followed here: www.themaddocblogs.com