Being able to rapidly identify an acute myocardial infarction (MI) pattern on the ECG is a vitally important skill for clinicians, particularly those that work front line in the Emergency Department. MI causes permanent damage to heart muscle and any delay in identification can lead to catastrophic results for the patient.
ST elevation myocardial infarction (STEMI) generally presents with characteristic cardiac chest pain. The ECG shows ST segment elevation and development of Q waves and cardiac enzymes are raised.
The ECG criteria for a STEMI are as follows:
- ≥ 2 mm of ST segment elevation in 2 contiguous praecordial leads
- ≥ 1mm in other leads (2 contiguous)
- An initial Q wave or abnormal R wave develops over a period of several hours to days.
Test your MI identification skills with the following ECG examples:
- ECG example 1
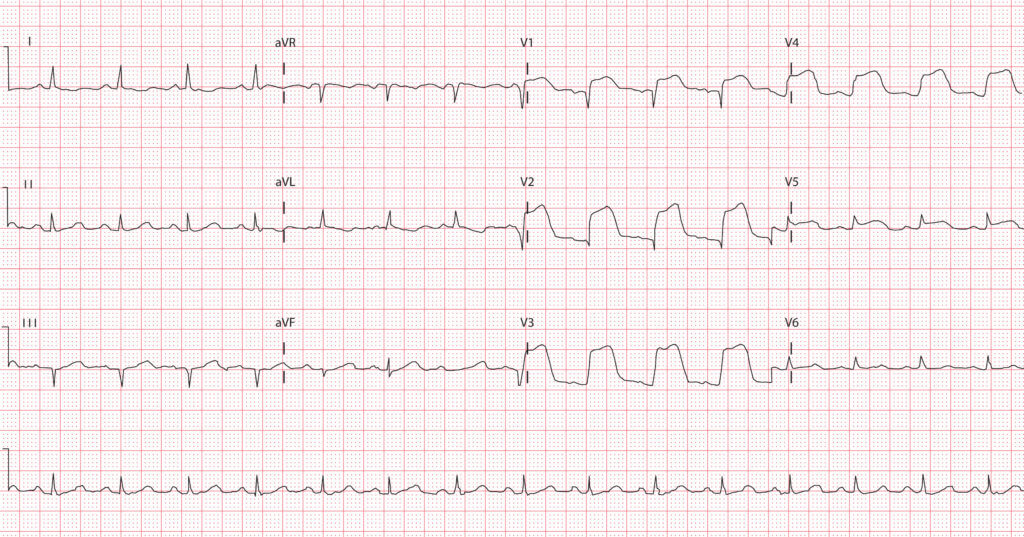
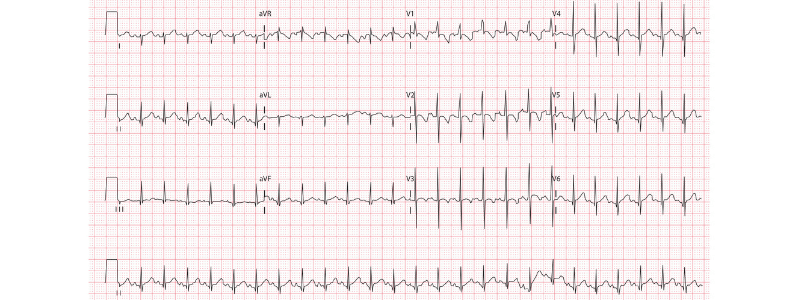
This is an extensive anterior MI, as demonstrated by the presence of:
- Massive ‘tombstone’ pattern ST elevation in leads V1-V4
- Less significant ST elevation in lead V5
- Q waves in leads V1 and V2
Anterior myocardial infarctions are usually caused by occlusion of the left anterior descending (LAD) coronary artery. The characteristic ‘tombstone’ pattern seen here is highly suggestive of a proximal LAD occlusion and is indicative of a large territory infarction with a poor left ventricular ejection fraction and a high likelihood of developing cardiogenic shock and death.
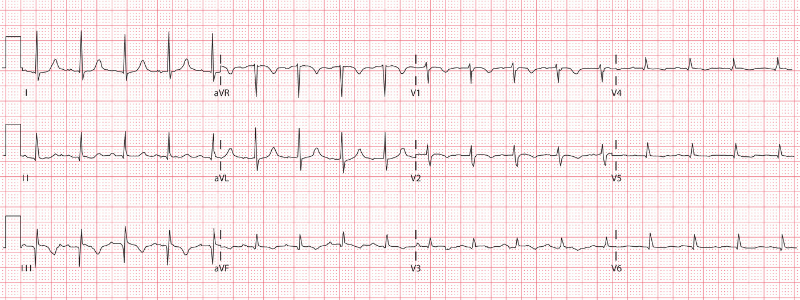
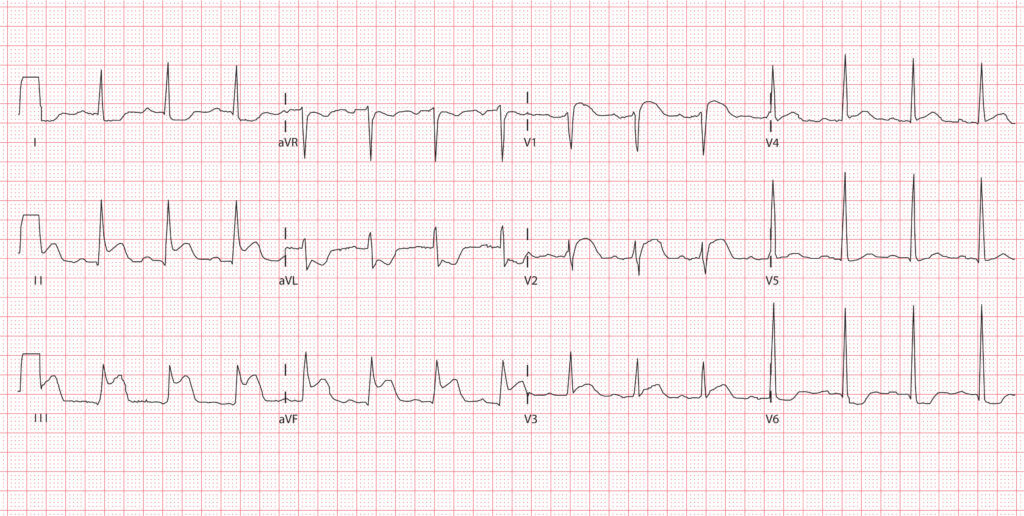
- ECG example 2
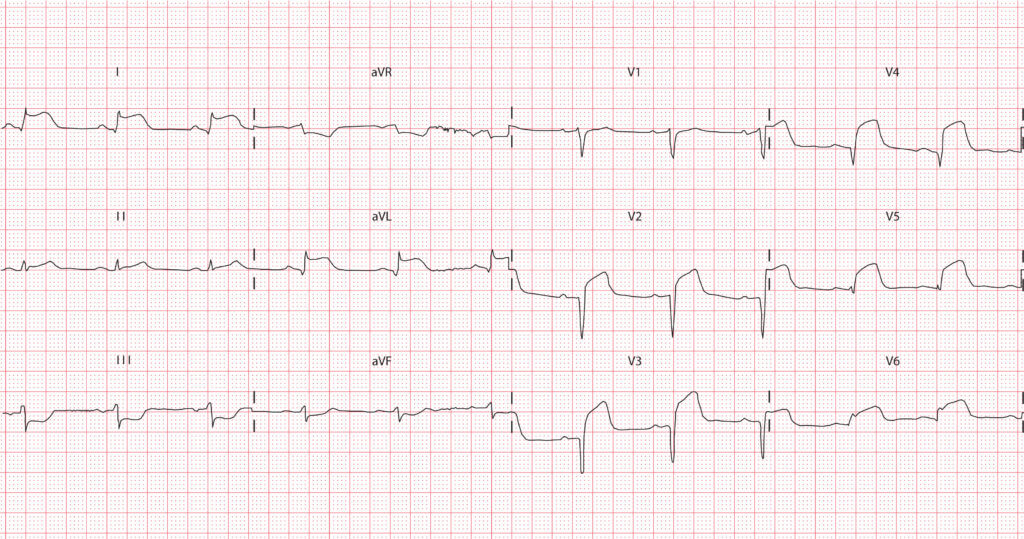
This is an acute anterolateral MI, as demonstrated by the presence of:
- ST elevation in leads I, aVL, and V2-V6
- Reciprocal ST depression in leads III and aVF
- Q waves in leads V2-V4
Anterolateral myocardial infarctions are usually caused by occlusion of the proximal left anterior descending (LAD) coronary artery, but can also be caused by combined occlusion of the LAD together with the right coronary artery or left circumflex artery.
- ECG example 3
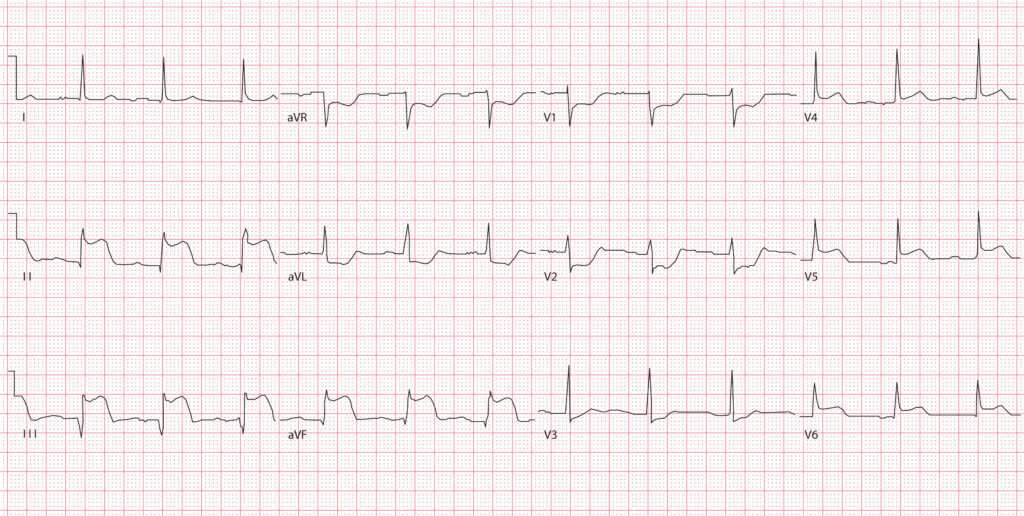
This is an acute inferior MI, as demonstrated by the presence of:
- ST elevation in leads II, III, aVF, and V4-V6
- Reciprocal ST depression in leads aVR, aVL and V1-V3
- Q waves in leads II, III and aVF
Inferior myocardial infarctions are usually caused by occlusion of the right coronary artery (in approximately 80% of cases), but can also be caused by occlusion of the left circumflex artery (in approximately 20% of cases).
- ECG example 4
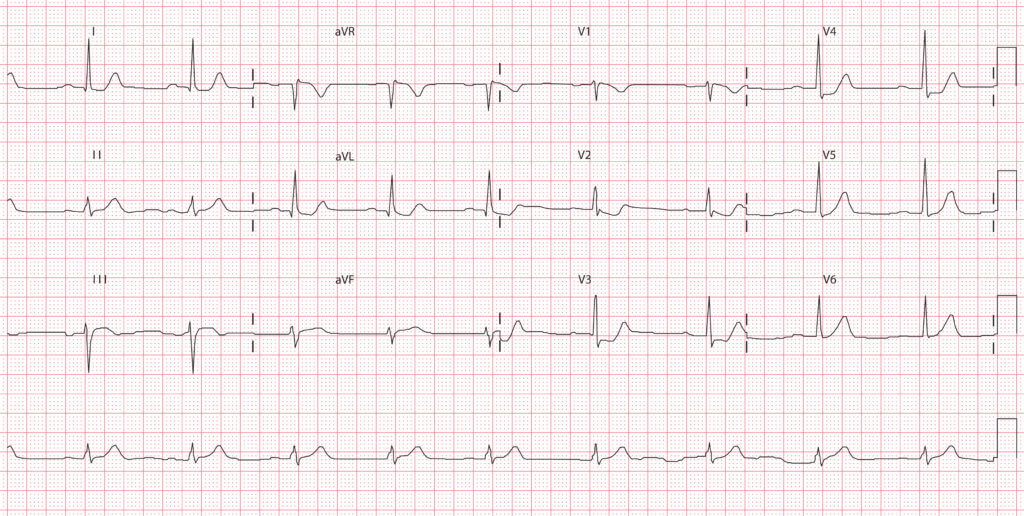
This is an acute posterior MI as demonstrated by the presence of:
- ST depression in leads V2 and V3
- Dominant R wave (R/S ratio >1) in lead V2
- Tall and broad R waves (> 30 ms) in leads V2 and V3
No ECG lead directly ‘looks’ at the posterior wall on a standard ECG. It is, however, possible to place the ‘posterior leads’ V7-V9 to assist with diagnosis. Lead V7 is placed at the level of lead V6 in the posterior axillary line, lead V8 on the left side of the back at the tip of the scapula, and lead V9 halfway between lead V8 and the left paraspinal muscles. When using posterior leads to diagnose a posterior MI, ST elevation in leads V7 through V9 is defined as elevation of at least 0.5 mm >2 of the leads.
The following ECG is performed in the same patient, this time with the ‘posterior leads’ in place:
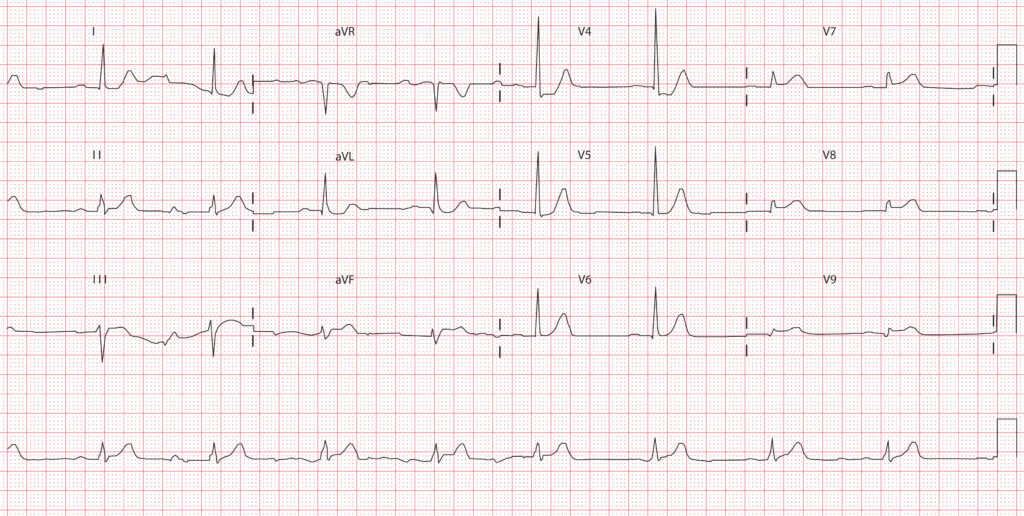
This time it can clearly be seen that there is greater than 0.5 mm ST elevation in leads V7-V9, confirming the diagnosis of a posterior MI.
Posterior myocardial infarctions are usually caused by occlusion of the right coronary artery.
- ECG example 5
This is an acute right ventricular MI, as demonstrated by the presence of:
- ST elevation in lead VI
- ST elevation greater in lead III than in lead II (as lead III is more ‘rightward facing’ than lead II and is more sensitive to right ventricular injury)
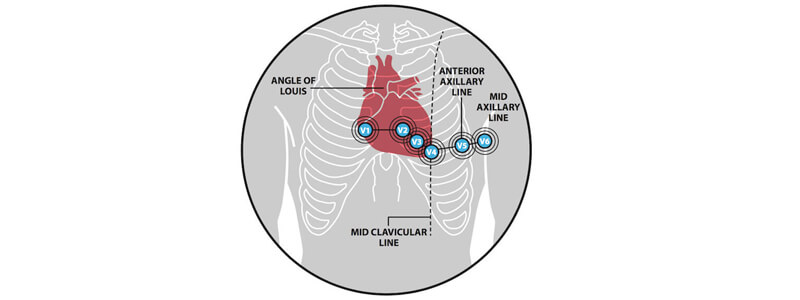
When an ECG is suggestive of a right ventricular MI it is possible to use a modified lead V4R to assist with diagnosis. The lead V4R is obtained by placing the V4 electrode in the 5th right intercostal space in the mid-clavicular line.
The following ECG is performed in the same patient, this time with lead V4R in place:
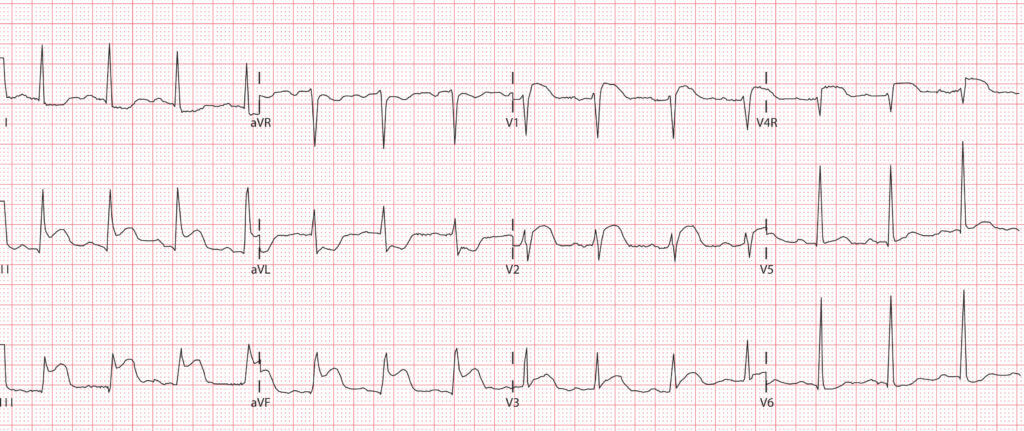
This time it can clearly be seen that there is significant ST elevation present in lead V4R, confirming the diagnosis of a right ventricular MI.
Right ventricular myocardial infarctions are usually caused by occlusion of the right coronary artery.